Vasa Previa – What You Need to Know as a Parent
Overview
Vasa previa is a condition where the baby’s blood vessels cross over the opening of the cervix (the entrance to the birth canal). These vessels carry blood directly to and from the baby, but unlike normal vessels, they are not supported by the placenta or uterine tissue. This makes them fragile and at risk of breaking when the water breaks or during labor. If these vessels tear, the baby can lose blood quickly, which can be life-threatening.
There are three types of vasa previa:
- Type I: The vessels come directly from an abnormal umbilical cord attachment called a velamentous insertion.
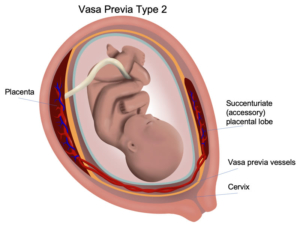
- Type II: The vessels connect separate parts of a bilobed or multilobed placenta (placenta with multiple lobes).
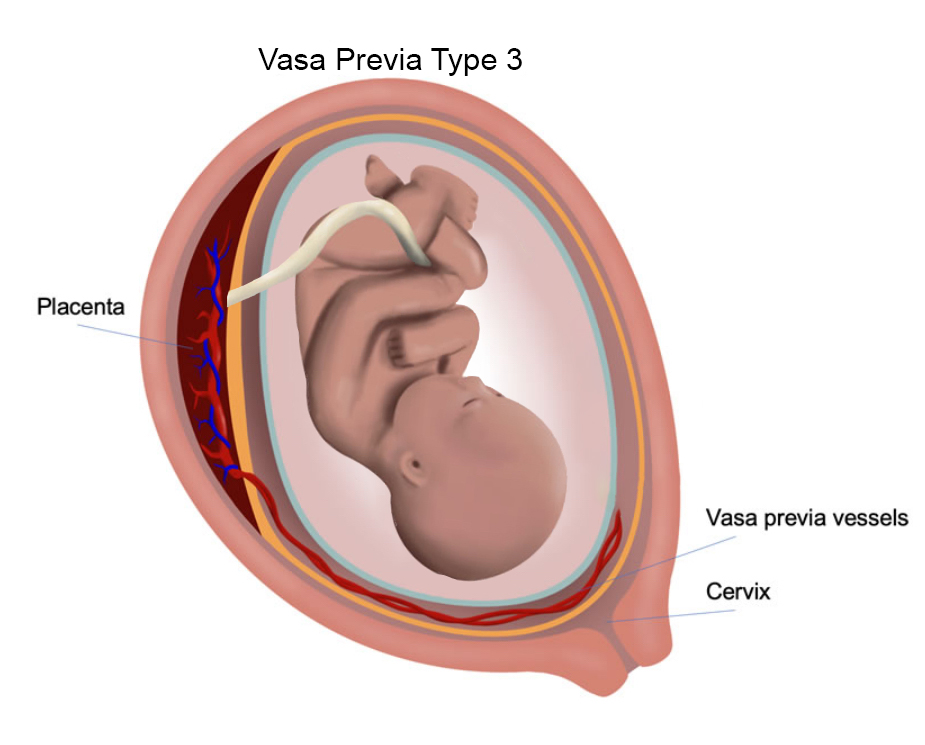
- Type III: The vessels run freely over the cervix but come from a normal-looking cord and placenta, making this type harder to detect.
Thanks to better monitoring and planned early cesarean delivery before labor begins, deaths related to vasa previa have dropped dramatically.
How Is It Diagnosed?
Vasa previa can often be seen on ultrasound, especially with special vaginal (endovaginal) ultrasound. This helps doctors see the position of the vessels near the cervix and identify the type of vasa previa.
Treatment Options
For Type II (and other types), options include:
- Expectant Management (Careful Monitoring):
- Hospital stay usually starts between 28 and 32 weeks to be close to emergency care if bleeding or rupture happens.
- About one-third of patients may experience vaginal bleeding during pregnancy, so constant monitoring is important.
- Steroid shots are given around 28 weeks to help mature the baby’s lungs in case early delivery is needed.
- Planned cesarean delivery is recommended at about 35 weeks before labor or water breaking to avoid vessel rupture.
- With prenatal diagnosis and close care, the risk of baby death drops from 40-50% to around 3%.
- Hospital stay usually starts between 28 and 32 weeks to be close to emergency care if bleeding or rupture happens.
- Operative Fetoscopy and Laser Ablation:
- A minimally invasive procedure using a tiny camera and laser to seal off the risky vessels crossing the cervix.
- This lowers the risk of sudden bleeding and death from vessel rupture.
- It may reduce or eliminate the need for long hospitalization and allow delivery closer to full term (after 35 weeks).
- A minimally invasive procedure using a tiny camera and laser to seal off the risky vessels crossing the cervix.
Risks include preterm rupture of membranes and preterm labor, common to invasive fetal procedures.
Vasa previa is an obstetrical condition in which fetal vessels cross over the internal cervical os. The cervical os is the opening from the womb to the birth canal, and is through which the baby is delivered vaginally. Because the vasa previa vessels are unsupported by underlying placenta, these vessels may be damaged if the bag of waters breaks or if the cervix dilates (opens) during labor. These vessels are directly connected to the baby. If these vessels break open, it can result in sudden blood loss and drop in blood pressure of the baby.
Vasa previa has historically been associated with high perinatal mortality rates due predominantly to fetal hemorrhage (bleeding) after vessel damage at time of membrane rupture. However, there has been a significant reduction of the perinatal mortality rate. This may be attributed to intensive monitoring of the pregnancy and subsequent preterm elective cesarean section timed to precede rupture of membranes.
Vasa previa has been classified into three types: Type I if the vasa previa arises directly from a velamentous umbilical cord insertion, Type II if it bridges separate lobes of a bilobed or succenturiate placenta, and Type III if it exits and reenters a single-lobed placenta without a velamentous cord insertion. Diagnosis and classification of a vasa previa is feasible by ultrasound evaluation of the lower uterine segment. Often endovaginal ultrasound will be necessary to confirm the diagnosis.
Patients with Type II or Type III Vasa Previa may be offered the following treatment options:
- Expectant management: The perinatal mortality rate for vasa previa has been historically quoted to be upwards of 40 to 50% due to unrecognized rupture of the fetal vessel and resultant fetal exsanguination. The perinatal mortality rate for prenatally recognized vasa previa may be as low as 3%. The rate of perinatal morbidity is unknown. Hospitalization for the duration of the pregnancy is usually recommended between 28 and 32 weeks gestation to maintain close proximity to the operating room in case of suspected rupture of the vasa previa. Because about one-third of patients may develop vaginal bleeding during the course of the pregnancy, timely identification of the source of bleeding and access to continuous fetal monitoring is required. Corticosteroids at 28 weeks for fetal maturation therapy is often given. Delivery is recommended without prior amniocentesis at 35 weeks gestation.
- Operative fetoscopy and laser ablation of the vasa previa. The potential benefit of this option is that risk of sudden fetal death from rupture of the vasa previa is substantially less. This option would also remove the diagnostic dilemma of vaginal bleeding. Prolonged hospitalization may be avoided, and delivery may occur beyond 35 weeks gestation. The risks of this option are those related to operative fetoscopy in general, such as preterm rupture of membranes and preterm labor. We typically perform laser ablation of the vasa previa at 31 to 33 weeks gestation.
For further reading, please see the link below: