Twin-Twin Transfusion Syndrome (TTTS) – What You Need to Know as a Parent
Overview
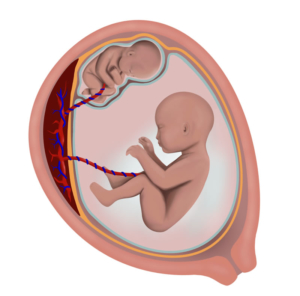
TTTS is a rare condition that affects about 10% of identical twins who share one placenta. In TTTS, blood flows unevenly between the twins through shared blood vessels. One twin (the donor) gives too much blood to the other (the recipient). The donor twin has low amniotic fluid and may not grow well, while the recipient twin has too much fluid, struggles with heart problems, and may develop swelling (hydrops). Without treatment, TTTS can lead to loss of one or both babies due to complications like heart failure or premature labor.
How Is It Diagnosed?
Doctors use ultrasound to confirm the twins share a placenta (monochorionic). They check the amount of amniotic fluid in each sac: the donor twin’s fluid is very low (less than 2 cm) and the recipient twin’s fluid is very high (8 cm or more). A staging system called Quintero helps describe the severity:
- Stage I: Donor twin’s bladder is visible on ultrasound.
- Stage II: Donor twin’s bladder is not visible.
- Stage III: Abnormal blood flow patterns seen in the twins.
- Stage IV: Fluid buildup/swelling (hydrops) occurs.
- Stage V: One or both twins have died.
Treatment Options and Outcomes
Without treatment, about 90% of pregnancies diagnosed with TTTS before 28 weeks may be lost. The main treatments are:
- Laser Surgery:
A thin camera and laser are inserted through a tiny incision in the mother’s belly. The laser seals off the shared blood vessels causing the uneven blood flow, stopping TTTS. This improves survival chances for both babies. Survival rates after laser treatment are approximately:
- Stage I: 92% chance at least one twin survives, 79% chance both survive
- Stage II: 93% one survives, 76% both survive
- Stage III: 88% one survives, 59% both survive
- Stage IV: 92% one survives, 68% both survive
- Stage I: 92% chance at least one twin survives, 79% chance both survive
- Expectant Management:
Watching carefully with frequent ultrasounds but no intervention. Unfortunately, this has about a 90% chance of pregnancy loss in severe cases. - Amnioreduction:
A needle removes excess fluid from the recipient twin’s sac to reduce pressure and prevent early labor. This doesn’t fix the blood flow problem, so fluid may build up again, requiring multiple procedures. - Umbilical Cord Occlusion:
Stopping blood flow to one twin to protect the other. This leads to the death of one twin and is not offered here because laser surgery is safer and aims to save both babies. - Pregnancy Termination:
An option up to about 24 weeks in some areas. - Other Procedures:
Fetal septostomy (making a hole in the membrane between twins) is not recommended because it can cause cord entanglement and worse outcomes.
Who Can Have Laser Surgery?
You may be eligible if:
- Your pregnancy is between 16 and 26 weeks.
- You have monochorionic twins with TTTS diagnosed by fluid levels (recipient sac fluid ≥ 8 cm, donor sac fluid ≤ 2 cm).
You may not be eligible if:
- One or both babies have major birth defects or genetic abnormalities.
- There is a hole purposely made in the membrane between twins.
- You have leaking membranes, infection, placental problems, or are in labor.
- You cannot commit to follow-up care.
What to Expect During Laser Surgery
The surgery is done with local anesthesia and sedation. A tiny incision (about 3 mm) is made to insert a small camera and instruments into the uterus. The surgeon finds and seals off the connecting blood vessels on the placenta with laser energy. Excess fluid may be drained afterward. Antibiotics are given to prevent infection.
After Surgery
You will likely stay in the hospital 1–2 days. After discharge, you will have weekly ultrasounds for the first month, then every 3–4 weeks until delivery. Your doctors will monitor your pregnancy closely and plan delivery based on your babies’ health.
Summary
TTTS is a serious condition where blood flows unevenly between identical twins sharing a placenta. Laser surgery can stop this abnormal blood flow and significantly improve survival and outcomes for both babies. Early diagnosis and close monitoring are key.
Twin-twin transfusion syndrome (TTTS) is a rare condition that afflicts about 10% of twins that share the same placenta (monochorionic twins). The cause of TTTS is attributed to unbalanced flow of blood through vascular channels that connect the circulatory systems of each twin via the common placenta. The shunting of blood through the vascular communications leads to a net flow of blood from one twin (the donor) to the other twin (the recipient). The donor twin develops oligohydramnios (low amniotic fluid) and poor fetal growth, while the recipient twin develops polyhydramnios (excess amniotic fluid), heart failure, and hydrops. If left untreated, the pregnancy may be lost due to lack of blood getting to the smaller twin, fluid overload and heart failure in the larger twin, and/or preterm (early) labor leading to miscarriage of the entire pregnancy. Treatment for TTTS consists of using laser energy to seal off the blood vessels that shunt blood between the fetuses. Because the surgical approach is via an operative fetoscope (a very thin instrument about the diameter of a straw), there is minimal risk to the mother. Laser therapy for TTTS has been shown to provide improved pregnancy outcomes compared to alternative therapies. Further information regarding pregnancy outcomes is detailed in the management options and outcomes section below.
Diagnosis and Staging
The in utero diagnosis of TTTS is established by ultrasound. First, the presence of a monochorionic twin gestation should be confirmed. Usually ultrasounds performed earlier in the pregnancy may be useful in establishing the chorionicity (number of placentas). Ultrasound findings such as a single placenta, same fetal sex, and a “T-sign” in which the dividing membrane inserts perpendicular to the placenta are helpful in diagnosing a monochorionic twin gestation.
TTTS is then diagnosed simply by assessing the discordance of amniotic fluid volume on either side of the dividing fetal membranes. The maximum vertical pocket (MVP) of amniotic fluid volume must be greater than or equal to 8.0 centimeters in the recipient’s sac, and less than or equal to 2.0 centimeters in the donor’s sac.
Once the diagnosis of TTTS is established, the severity of the condition may be assessed using the Quintero Staging System, as listed below. This staging system is based on the observations of several hundred patients with TTTS. Not only does this staging system mirror the progression of disease, but it has also been shown to be important in establishing the prognosis. An atypical presentation of TTTS may occur if the fetal bladder of the donor twin remains visible despite the presence of critically abnormal fetal Dopplers or hydrops.
Quintero Staging System
Stage I: The fetal bladder of the donor twin remains visible sonographically.
Stage II: The bladder of the donor twin is collapsed and not visible by ultrasound.
Stage III: Critically abnormal fetal Doppler studies noted. This may include absent or reversed end-diastolic velocity in the umbilical artery, absent or reverse flow in the ductus venosus, or pulsatile flow in the umbilical vein.
Stage IV: Fetal hydrops present.
Stage V: Demise of either twin.
Management Options and Outcomes
Untreated, TTTS that presents before 28 weeks gestation is associated with approximately 90% perinatal mortality rate. Because of the dismal prognosis of TTTS, various treatment methods have been advocated. Recent studies have shown improved outcomes in patients treated with laser therapy compared to the traditional method of serial amnioreductions. The treatment options along with expected pregnancy outcomes are listed below.
- Laser Surgery: This surgical approach utilizes an operative fetoscope to deliver laser energy that then seals off the offending blood vessels on the surface of the common placenta. Because the vascular connections between the two fetuses are sealed, no further blood exchange between the fetuses takes place, thus eliminating the syndrome. Pregnancy outcomes after laser therapy for TTTS depends on the stage of the disease. According to our study of 682 cases of laser surgery, the perinatal survival after laser surgery for TTTS is as follows:
Perinatal Survival Stage I (n=122) Stage II (n=177) Stage III (n=328) Stage IV (n=63) At Least 1 Twin Survival 92% 93% 88% 92% Dual Twin Survival 79% 76% 59% 68% - Alternative Therapies: Possible management alternatives for TTTS include the following:
- Expectant Management – In this option the pregnancy would be followed with serial ultrasound examinations. There is approximately a 90% pregnancy loss rate in advanced cases of TTTS diagnosed before 28 weeks gestation.
- Amnioreduction – The purpose of this procedure is to remove excess amniotic fluid from the recipient’s sac in order to prevent premature birth or miscarriage. This procedure is done via a needle placed using ultrasound guidance. Because this approach does not treat the underlying cause of TTTS, amniotic fluid excess may recur, resulting in the need for multiple amnioreductions.
- Umbilical Cord Occlusion – This procedure utilizes an operative fetoscope to interrupt the flow of blood through the umbilical cord of one of the fetuses. This fetus dies and remains inside the uterus for the duration of the pregnancy. Because the risks of this procedure are similar to laser therapy, but laser therapy provides the additional benefit of the chance of survival for both twins, this procedure is not offered for the treatment of TTTS at this center.
- Interruption of the Pregnancy – Pregnancy termination may be chosen as an option up to 24 weeks gestation in California. We do not offer this procedure.
- Other – Fetal septostomy has been suggested as a treatment option for TTTS. This procedure entails the purposeful needling of the dividing membrane in the hopes to equalize the amniotic fluid within each sac. Studies have not shown improved outcomes using this approach. Moreover, the disruption of the dividing membrane may result in cord entanglement, which may be an additional cause of fetal death. We advise against this procedure. If this procedure has been purposely done, you will not be a candidate for laser surgery.
Who is a Candidate for Laser Surgery
To qualify for laser surgery, the following criteria must be met:
Inclusion Criteria
- Gestational age: 16 weeks 0 days to 26 weeks 0 days.
- Diagnosis of TTTS:
- Single (shared placenta) with thin dividing membrane (or no dividing membrane in the case of monoamniotic twins)
- Polyhydramnios: maximum vertical pocket of 8 centimeters or more in the recipient twin, prior to amnioreduction
- Oligohydramnios: maximum vertical pocket of 2 centimeters or less in the donor twin, prior to amnioreduction
Exclusion Criteria
- One or both babies have other major birth defects.
- Genetic studies showing an uncompensated abnormality.
- A hole in the dividing membrane that was intentionally made.
- Ruptured fetal membranes (leakage of amniotic fluid from the vagina).
- Chorioamnionitis (infection in the uterus).
- Ultrasound evidence of brain damage of either fetus.
- Placental abruption (separation of the placenta from the uterus).
- Active labor.
- Unable or unwilling to participate in observational study or to be followed up.
Laser Surgery – Details of Procedure
All surgeries are performed under local anesthesia with some intravenous sedation. A small incision (3 millimeters or about 1/10th of an inch) will be made and a trocar (small metal tube) will be inserted into the amniotic sac of the recipient twin. Amniotic fluid may be sent for genetic and microbiology studies. An endoscope (medical telescope) will be passed into the uterus. The blood vessels, which are visible on the surface of the placenta, will be analyzed, and all communicating vessels will be sealed off with laser energy. A second trocar may have to be inserted to complete the surgery, particularly if the placenta is anterior. At the conclusion of the surgery, the excess amniotic fluid may be drained from the sac of the recipient twin. You will be given antibiotics before and after surgery.
Laser Surgery – Postoperative Care
Typically, you will remain in the hospital for 1 to 2 days after surgery. You will then be sent home to the care of your primary obstetrician and perinatologist. Weekly ultrasound is recommended for the four weeks after surgery. Then, depending on the clinical circumstances, follow up ultrasounds may be performed every 3 to 4 weeks for the duration of the pregnancy. Details of the delivery and information regarding the health of the infants will be requested.
For further reading, please see the link below: