Open Spina Bifida / Myelomeningocele – What You Need to Know as a Parent
Overview
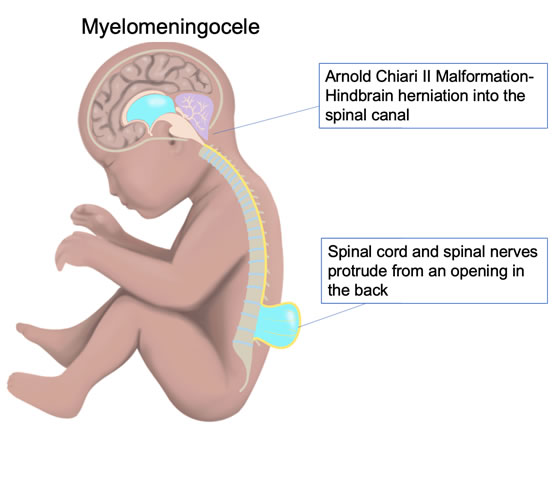
Open spina bifida is a birth defect that happens when the baby’s spine doesn’t fully close during development in the womb. This causes the spinal cord and its covering membranes to stick out through the opening in the spine. The most common type is called myelomeningocele (MMC). In some cases, the spinal cord is exposed without any covering, which is even more severe.
This condition often leads to problems with the brain, called Arnold Chiari II malformation, where part of the brain pushes down into the spinal canal. This can block the normal flow of fluid around the brain and cause a buildup called hydrocephalus.
Because the exposed spinal cord can get damaged by fluid in the womb and ongoing trauma, repairing the defect before birth may help improve the baby’s function after birth.
How Is It Treated?
There are several options:
- Waiting until after birth for repair: This avoids risks to the mother during pregnancy but allows ongoing damage to the spinal cord before birth.
- Termination of pregnancy: An option before a certain gestational age in some places.
- Open fetal surgery: This is a surgery done during pregnancy where the mother’s abdomen and uterus are opened to repair the baby’s spine. A large study showed this helps reduce the need for brain fluid shunts, improves brain structure, and improves the baby’s ability to walk. However, it carries significant risks including early labor, uterine rupture in this or future pregnancies, and other complications.
- Minimally invasive fetoscopic surgery (keyhole surgery): This newer technique uses small instruments inserted through tiny incisions to repair the baby’s spine without opening the uterus. It lowers risks to the mother and allows for vaginal delivery, while still offering benefits to the baby. There are two types:
- Percutaneous: Instruments go directly through the abdomen and uterus. Faster recovery but higher risk of early water breaking and preterm birth.
- Laparotomy with uterine exteriorization: The uterus is brought outside the abdomen to allow surgery, with a longer recovery and abdominal scar but lower risk of early water breaking.
- Percutaneous: Instruments go directly through the abdomen and uterus. Faster recovery but higher risk of early water breaking and preterm birth.
Who Is a Candidate for Surgery?
You may be eligible if:
- Your baby has myelomeningocele or myeloschisis between spinal levels T1 and S1, with evidence of brain hindbrain herniation. Patients without hindbrain herniation will be assessed on a case-by-case basis.
- You are 18 years or older.
- Your pregnancy is between 19 and about 28 weeks.
- Genetic testing and fetal heart ultrasound are normal.
- You pass social work and pediatric neurology evaluations.
- You can stay near the treatment center for follow-up.
You may not be eligible if you have:
- Twins or multiples.
- Diabetes requiring insulin before pregnancy.
- Other major fetal defects.
- Certain uterine or placental problems.
- High BMI (40+).
- History of early preterm birth.
- Infections like HIV or Hepatitis.
- Other factors that could affect your or your baby’s health or ability to follow-up.
After Surgery
You will stay in the hospital for about 2 days. After going home, you’ll need to rest and limit activity, staying close to the hospital for regular check-ups every 1–2 weeks. About 4 weeks after surgery, a detailed MRI of the baby will be done to check repair results.
Depending on your situation, vaginal delivery may be possible. After birth, your baby will be cared for at a specialized children’s hospital with follow-ups scheduled at 6, 12, 24, 30, 48, and 60 months of age.
Open spina bifida occurs in approximately 1 in 1,500 births annually in the United States. Open spina bifida develops when the spine fails to close at some point along its length during fetal development. Failure of the vertebrae, the bony part of the spinal column, to close around the spinal cord results in different forms of spina bifida. Myelomeningocele (MMC) is the most common type and occurs when both the meninges (membranous coverings) and the spinal cord protrude through the spinal defect. Myeloschisis is the most severe type and occurs when the spinal cord protrudes with no meninges covering the defect. These forms of spina bifida are oftentimes accompanied by a condition known as Arnold Chiari II Malformation, or herniation of the hindbrain (brain stem). When cerebral spinal fluid (CSF) escapes from the open spinal defect, it causes the hindbrain to descend into the spinal canal. This blocks CSF circulation and may lead to hydrocephalus, or accumulation of CSF in the brain.
MMC leads to injury and loss of spinal cord tissue at and below the defect. The abnormal spinal cord development, intrauterine trauma, and the toxic exposure to amniotic fluid may contribute significantly to the newborn’s neurological status (“two-hit hypothesis”). Because of these in-utero factors, fetuses with open spina bifida may benefit from correction before birth to improve function after birth.
In 2003, the NIH sponsored a multi-center randomized controlled trial of in utero repair of MMC vs. standard neonatal repair, the Management of Myelomeningocele Study (MOMS), the results of which were published in 2011. Prenatal repair resulted in reduction of the need of shunting at 12 months of age, decreased rate of hindbrain herniation by one-third at 12 months, doubling of the ability to ambulate without the assistance of orthotics, and produced a level of function that was two or more levels better than expected according to anatomic levels. However, the in utero repair was performed via open maternal-fetal surgery, which means the mother’s abdomen is opened (laparotomy) and her uterus is opened (hysterotomy), and was associated with significant risks, including higher rates of preterm birth, fetal bradycardia, oligohydramnios, placental abruption, pulmonary edema, maternal transfusion at delivery, and a 35% risk of uterine thinning or dehiscence or rupture. Furthermore, the legacy of open in utero repair in regards to a patient’s future pregnancies is an approximately 28% risk of uterine dehiscence or rupture.
Our group has worked on developing a minimally-invasive technique (so-called ‘keyhole surgery’) for the antenatal treatment of MMC, translating an experience of more than 10 years in the animal model to a viable clinical application. The technique developed by our group does not require hysterotomy (uterine incision). Rather, small instruments are placed into the womb through tiny incisions, and with the use of partial CO2 insufflation, the open spina bifida is repaired. This approach minimizes the risks of the surgery for the mother, while preserving the potential benefits of the in utero repair for the fetus.
The following management options will be offered to all eligible patients.
Management Options
- Expectant management with standard postnatal repair. This option provides minimal maternal risks and low risk of preterm birth. Yet, it may result in progressive deterioration of nerve tissue due to continued intrauterine trauma and exposure to the toxic effects of amniotic fluid.
- Termination of pregnancy.
- Prenatal repair of the myelomeningocele via open maternal fetal surgery. This approach requires maternal laparotomy and hysterotomy, under deep general anesthesia. This is the approach used in the Management of Myelomeningocele Study (MOMS).
- Fetoscopic prenatal repair. The primary benefit of this approach is the lessened maternal risks as compared to the open maternal fetal surgical approach. Also, vaginal delivery is acceptable for this and future pregnancies. There are two fetoscopic techniques, percutaneous and laparotomy/uterine exteriorization, described below.
Who is a Candidate for Surgical Treatment?
Inclusion Criteria
- Myelomeningocele (including myeloschisis) beginning at level T1 through S1 with hindbrain herniation. Patients without hindbrain herniation will be assessed on a case-by-case basis.
- Maternal age ≥18 years
- Gestational age of 19 to 27 6/7 weeks
- Normal karyotype and/or microarray
- Normal echocardiogram
- Positive evaluation of social work consult
- Positive evaluation from pediatric neurology consult
- Willing to remain in the area for post-surgical follow-up and delivery, and be willing to return to our center for postdelivery evaluations.
Exclusion Criteria
- Multiple gestation
- Insulin-dependent pre-gestational diabetes
- Presence of a fetal anomaly not related to myelomeningocele
- Fetal kyphosis ≥ 30 degrees
- Presence of uterine cervical cerclage or incompetent cervix
- Placenta previa or placental abruption
- Short cervix < 25 mm
- BMI of 40 or greater
- History of preterm delivery prior to 37 weeks
- Maternal-fetal Rh isoimmunization, Kell sensitization, or neonatal alloimmune thrombocytopenia
- Maternal HIV, Hepatitis-B, Hepatitis-C status positive
- Negative psychosocial evaluation as determined by the social worker
Details of Procedure
We offer two fetoscopic approaches to correcting the open spina bifida defect, both of which require general anesthesia and a 2-day inpatient stay:
- Direct percutaneous – In the minimally-invasive direct percutaneous method, 3-4 ports are placed percutaneously through the maternal abdomen and uterus. Amniotic fluid is removed and CO2 is placed into the womb. Dissection around the placode allows the placode to drop into the spinal canal. A dura patch is placed over the defect and the skin (and underlying muscle if possible) is reapproximated and sutured over the patch. If there is insufficient amount of skin to cover the defect, a secondary (skin) patch will be sutured into the skin to create a watertight seal (See Video below). Postoperative recovery is relatively quick and there is no laparotomy scar. Yet, this approach is associated with a relatively increased risk of preterm premature rupture of membranes (PPROM) and preterm birth.
- Laparotomy/Uterine exteriorization. In the laparotomy and uterine exteriorization method, an incision is made into the abdominal cavity and the uterus is exteriorized (removed out of the maternal abdomen). Two to three ports are placed through the exteriorized uterus and the procedure proceeds as previously described. The approach is associated with relatively increased postoperative recovery, a laparotomy scar, and possibly a higher anesthetic risk. Yet, this approach is associated with relatively decreased risk of PPROM and preterm birth.
Percutaneous Fetoscopic Closure of Open Spina Bifida Defect
Postoperative Care
You will remain in the hospital for about 2 days after surgery. You will then be sent home and asked to maintain minimal physical activity. This entails remaining at home for the duration of your pregnancy, except for doctor visits. You will have alternate follow-up visits between our office and your referring maternal-fetal medicine doctor every 1-2 weeks. You will also have a follow-up fetal MRI about 4 weeks after surgery. You may be given the option of a vaginal delivery, based on obstetric indications. Following delivery, your baby will be transferred to Children’s Hospital Los Angeles (CHLA) for management. Postnatal testing will be performed at CHLA at 6, 12, 24, 30, 48, and 60 months of age.
For further reading, please see the link below: